This 36 years old patient is from Provo Utah and t had a TVT sling, laparoscopic hysterectomy, anterior and posterior repair in 2016. She had the TVT retropubic sling for stress urinary incontinence. Since that time, she has had problems with pain in her groin, vagina and lower back. She also complains of pain with intercourse (aka dyspareunia). She had none of these symptoms prior to the 2016 surgery. She has been told by numerous surgeons, doctors and healthcare professionals that either the mesh was not removable or the mesh was not causing her pain.
After further discussion, the patient shows Dr Miklos her pain is not in the groin but instead the lower abdomen i.e. pubic area. She is especially sensitive over her right-side incision site in her pubic area. She also describes pain in the back of her legs. She described her pain in the lower abdomen as being 3-4/10 constantly and with exertion can go as high as 8/10. She explained that vaginal pain as being 3/10 at rest and 8/10 with attempts at intercourse. She has attempted pain medications, physical therapy and myofascial massage without relief of her pain.
She expresses that she feels she is getting some type of auto immune response – as her overall body aches. Recent lab tests reveal an elevated ANA level and she has a rash on her neck which is sun provoked. She has pain with sex with insertion and thrusting.
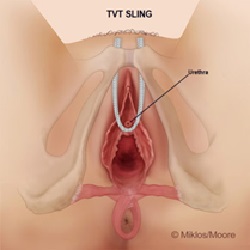
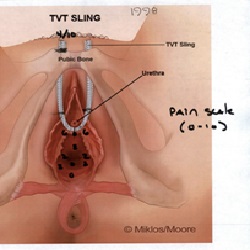
Her examination revealed that most pain was over the TVT mesh pathway (Figure 1). A blinded visual pain analog scale was used to determine her pain in each of the areas as shown (Figure 2). She also had a palpable mass on the right side of her pubic area which Dr Miklos expressed he believed was the TVT sling mesh and on exam her pain was described as 4/10. Please note the maximum amount of vaginal pain is along the TVT sling pathway. Other areas of the vagina, without mesh, are also painful. This is a common occurrence with mesh specific pain. Dr Miklos explained to the patient the risks and benefits of mesh removal as well as alternatives. She chose to have her mesh removed.
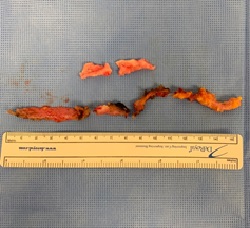
The surgery was performed through a vaginal and laparoscopic approach. This is by far the most successful way to remove the whole / complete TVT retropubic sling. A complete TVT removal is impossible through a vaginal incision alone. To remove a TVT sling the area above the vagina and bladder must be approached from the top down i.e. through the abdomen/pelvis. This approach give the best access to the sling and its attachment to the abdominal wall. (Figure 3) Her surgery was performed without complications and with an estimated blood loss of 1 tablespoon. The next morning after surgery the patient was already claiming that most of the areas of pain she had pre-surgery were gone. She explained that she does suffer from surgical site pain she feels this is completely different than where the mesh was anchored. Dr Miklos & Moore removed more than 25 cm of mesh (approximately 10 inches). (Figure 4) She was discharged the day after surgery claiming the surgery “was a success”.